

A Tale of Two Regimes of Dying
A Tale of Two Regimes of Dying
Or, The Difference a Bend of the Arm Makes
Canada continues its journey (fraught as it is) toward becoming one of the most permissive societies for assisted suicide and euthanasia (ASE).1 In spring of 2024, they plan to expand the offer to those people with mental illness. What does it look like to assess someone and make a determination whether they should be prevented from killing themselves or helped to do so? I have no idea, but clinicians in Canada are going to do it.
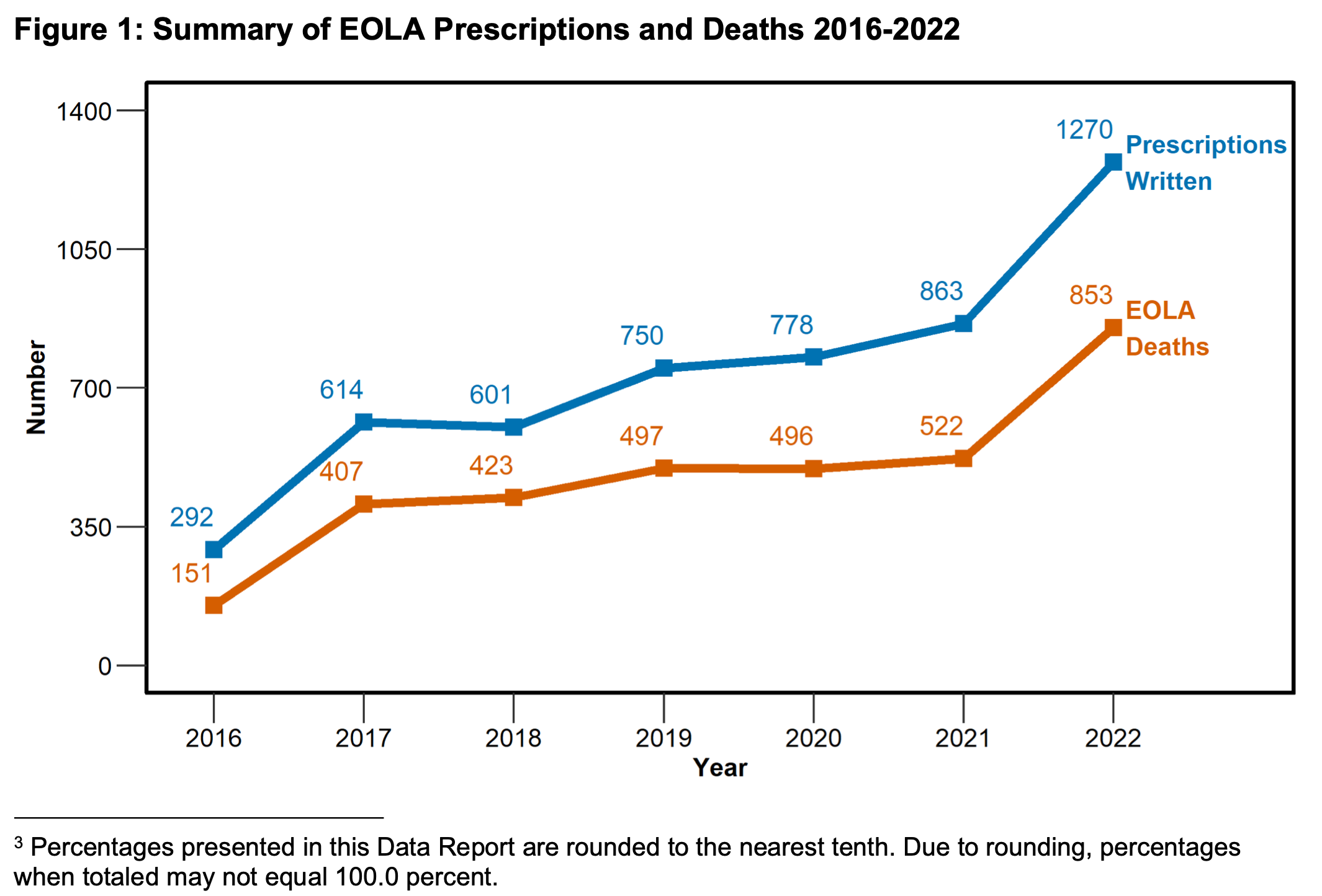
California is a jurisdiction worth contrasting with Canada because they have a similar total population and legalized ASE around the same time, yet they’ve produced vastly different results. Here’s the latest data from California:
And the latest data from Canada:
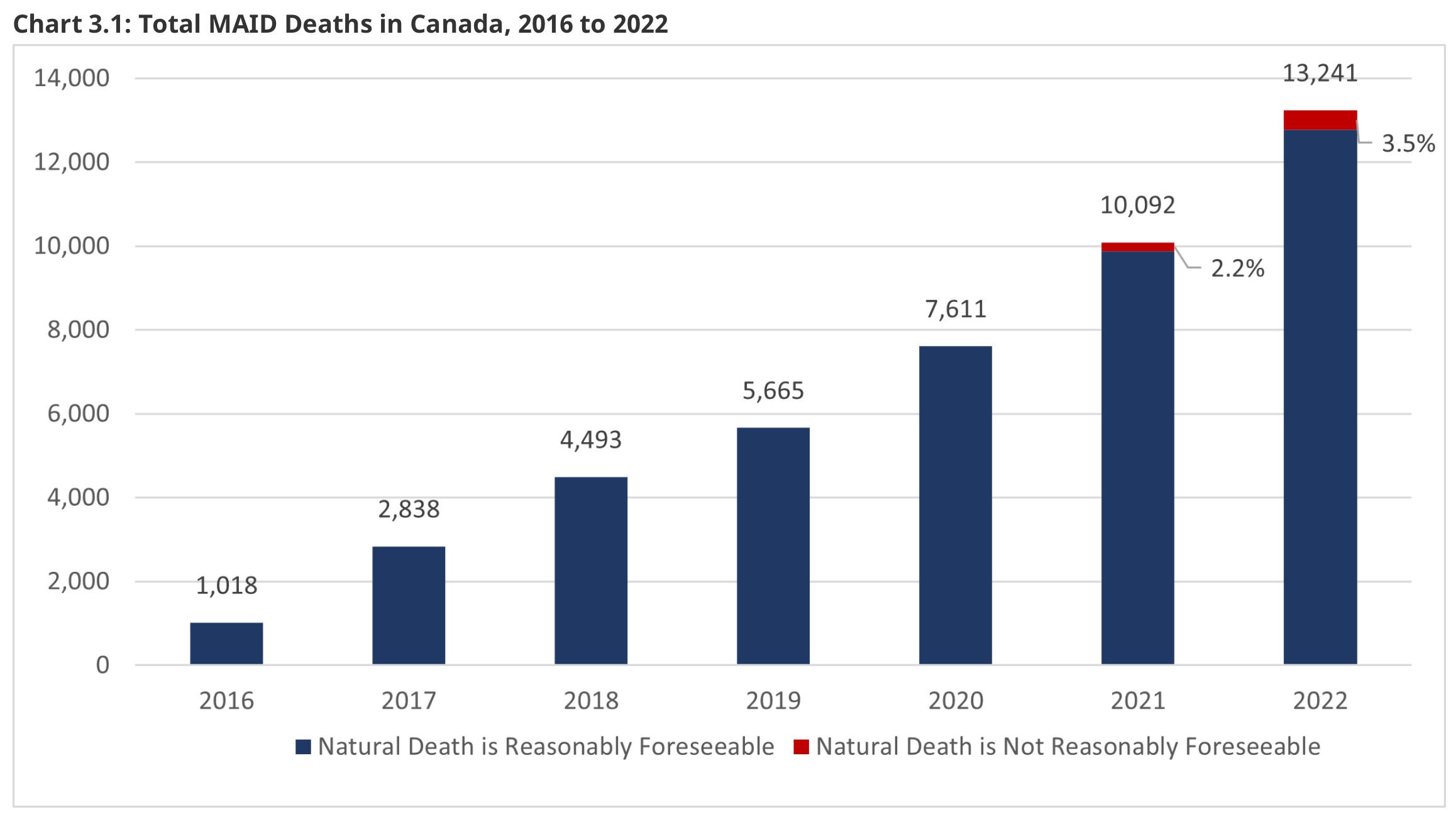
In 2022, ASE accounted for 4.1% of all deaths in Canada (the sixth leading cause of death in the nation). What’s happening in Canada to make this such a popular option? Or, what’s happening in California to restrain its use? As you can tell just from the presentation of the data, Canada offers ASE to some people who would never qualify for it in California - e.g., those whose natural death isn’t reasonably foreseeable. But that’s only 3.5% of the total (which is still ~463 people. not a small number, but not enough to account for the difference here). That doesn’t seem to be the reason why the numbers are so different.
While there have been some dramatic stories of people availing themselves of ASE in Canada for inadequate social supports, it would be hard to believe that these constitute a substantial number of the total. But then again, it would have been hard to believe that Canada would develop this kind of program over so short a period of time.
Perhaps you might think religion plays a role, but the religious demographics between the two jurisdictions are similar: 72% of Californians and 68% of Canadians have some kind of religious faith. There’s an interesting line of theological inquiry here for another time about how one considers ASE, but I don’t think we can pin the differences in practice on religious belief.
A more likely possibility is that the prognostic criteria are different. In California, one must have an incurable, irreversible condition that will result in death in less than six months. In Canada, for the majority of cases, someone’s natural death must be “reasonably foreseeable” (until recently anyway, but those receiving ASE without a reasonably foreseeable death remain a minority). Canadian authorities appear satisfied with a liberal interpretation of that criterion; you needn’t be eligible for hospice to be eligible for ASE in Canada.
Yet another possibility that could explain the difference between the two jurisdictions is that euthanasia is legal in Canada whereas it is not in California. Canada’s report indicates fewer than seven deaths resulted from self-administration of the lethal medication in 2022. Even among those who receive the lethal prescription in California (as in all US jurisdictions), many fewer go on to actually end their life using it. Someone may become too weak to self-administer the medication (and no assistance is currently allowed in the US). They may change their mind after receiving the medication. People who might opt for euthanasia, if it were legal, would never opt for assisted suicide. After all, the psychological barrier to ending one’s own life is immense, even when under great duress. Euthanasia, although it requires consent, might be experienced as a more passive procedure. It’s also more medicalized, which lends the assurance and authority to the event.
Combine these two things together - looser prognostication requirements and the permissibility of euthanasia - and you’ve got yourself a juggernaut of an ASE regime. The slope of that graph from Canada shows no signs of slowing. Once the rationale of death as a medical intervention is operative in a culture, it changes everything. Canada’s ASE regime remains in its infancy; who knows what it will look like in its maturity.
Alex Smith and Eric Widera recently hosted Bill Gardner, Leonie Here, and Sonu Gaind to discuss this issue. I’d recommend listening; it’s an insightful conversation:
Lessons from Canada
What might we infer from this? There’s a growing push to loosen safeguards around assisted suicide in US jurisdictions; indeed, safeguards are increasingly seen as barriers to access. I’m not sure what will happen as safeguards around waiting periods and residency requirements are eroded, but tampering with safeguards around prognostication or the method of killing will, I worry, substantially expand the use of death as a medical intervention. What is the final legal and clinical arrangement that will satisfy proponents in the US? Will it be a program as liberal as Canada’s? Do they really believe a tweak to a residency requirement or a waiting period is all that’s needed, and they’ll stop lobbying for legislative change thereafter?
It’s hard for me to interpret that advocacy charitably. Either proponents are naive or aren’t arguing in good faith. They may be naive because they fail to appreciate both the culturally formative and the legal power of precedent. Once your toe is in the water, it’s easier for the foot, leg, and whole body to dive right in. Once you justify A1, the case for justifying A2 becomes stronger, even if you can’t yet justify C. As Bill Gardner points out on GeriPal, when you draw a line, there will always be someone just on the other side of that line that you could reasonably justify including - and you keep moving the line in that way.
But maybe, if I understood advocacy arguments uncharitably, they’ve adopted an incrementalist approach. Maybe they hope to get the practice legalized with the standard safeguards, and then gradually pick apart the safeguards in the subsequent years, and “expand access” via other legal challenges (e.g., ADA challenges around self-administration). We see a similar push around “advance directives for dementia,” with clauses built in on when and how to deny someone food and water so that they’ll die once they reach a certain threshold of dementia severity. Do we really think we’ll be able to hold the line at denying people with dementia food and water when a rapid, effective means of killing is available via euthanasia? Once killing people in this way is normalized, compassion (albeit without wisdom) opens the door to ending the lives of people with dementia in other ways.
The legal histories of Canada and the United States are very different, and the Supreme Court of the United States on multiple occasions has not found a right to assisted suicide in our Constitution (e.g., Vacco v. Quill, Washington v. Glucksberg), contrary to Canada’s Supreme Court. However, Supreme Courts can reverse previously decided, seemingly bedrock opinions (e.g., Carter v. Canada overturning Rodriguez v. British Columbia in Canada, Dobbs v. Jackson Women’s Health Organization overturning Roe v. Wade in the US). For now, proponents in the US will continue a state-by-state approach, but for how long can they ignore the alarms in Canada?
Why do I refer to the practice as ASE and not MAID? Phillip Reed argues well that we should call assisted suicide what it is and avoid euphemism. I explain more here.
Thank you so much for your work on this, Josh.
Thank you Josh for this sober and accurate analysis of what’s happening with MAID and ASE. Not mentioned in your argument but ever more salient is that it is a lot cheaper to help someone die than to care for them. Exploding aging and seriously ill population = dangerous incentives.